by J. Haas, L. Bellows* (7/14)
Quick Facts…
- Osteoporosis is a process of severe bone deterioration resulting in a high susceptibility to bone fractures.
- It is most often seen in postmenopausal women, particularly light-skinned, small-framed women with a family history of osteoporosis.
- The loss of calcium from bones is the major effect of aging on the skeletal system.
- Therapies include estrogen replacement, prescriptive medications, physical activity and calcium supplements with or without additional nutrients. Such treatments can slow the rate of bone loss but not form new bone.
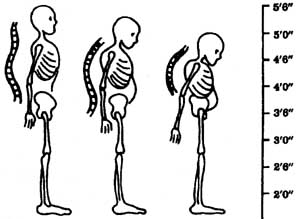
Figure 1: As the skeleton grows increasingly fragile, bone fractures, “dowager’s hump,” and loss of height may occur. |
Osteoporosis, the “brittle bones” disease, is caused by low bone mineral density (BMD). BMD is the measure of the density of minerals such as calcium in the bones. Peak BMD is usually reached by 30 years of age or so, and with age BMD begins to decrease. When BMD falls sufficiently below healthy values, low bone mass, or osteopenia, occurs. Osteoporosis occurs when BMD falls evenfurther, and it is so low that the skeleton is unable to sustain ordinary strains. As BMD falls, bone fractures, “dowager’s hump”, and loss of height may occur. See Figure 1.
Osteoporosis Risk Factors
This complex condition is a major debilitating disease that affects 20 to 30 percent of women over age 60. Osteoporosis, meaning “porous bones,” occurs earlier and with greater frequency and severity in women than in men; affecting an estimated 8 million women and 2 million men in the United States.
Men and women over 60 years old are at higher risk of osteoporosis than younger people. Nonetheless, it is possible to have osteopenia or osteoporosis at a much earlier age. Osteoporosis is seen most often in small-framed women, particularly white and Asian women, age 50 or older. These women have lower initial bone mineral content (BMC) and thus lighter bones at the onset of maturity than men or large-framed women. Not only are the bones of many women lighter than those of men, but loss of this bone accelerates at meno-pause, particularly the first three years after menopause.
Other factors associated with increased risk of osteoporosis include a family history of the disease, removal of the ovaries at an early age, cigarette smoking, excessive use of alcohol, inadequate intake of calcium, hormonal imbalances, certain medications (glucocorticoids and some anticonvulsants) and insufficient physical activity.
It is estimated that one in two women and one in four men over age 50 will eventually suffer an osteoporosis-related fracture at some point in their lifetime. Americans spend more than 19 billion dollars each year repairing some 2 million fractures resulting from osteoporosis. Osteoporotic-related fractures may be responsible for chronic pain, reduced quality of life, long term care admission, health care costs, mortality, and morbidity. Chances of surviving a broken hip or wrist are good, but many survivors are incapacitated and one in four dies within a year following the fracture.
Osteoporosis Diagnosis
Technology is available to determine bone mass (or density) safely, conveniently, and at relatively low cost. A BMD test is considered the best way to check your bone health. Dual-Energy X-Ray Absorptiometry (DEXA) assesses bone mineral density, and is available in most hospitals and many clinics. In combination with biochemical measurements, it is used to guide osteoporosis treatment.
For people at high risk of osteoporosis, health care programs designed to detect early osteoporosis are well worth the investment. They do not, however, replace nutrition and physical activity programs designed to retard the disease by strengthening bone mass.
Osteoporosis Treatment
Hormonal Replacement
Estrogen replacement therapy has been used to treat osteoporosis in postmenopausal women with variable results. The decrease in estrogen production signaling menopause causes an increase in the normal rate of bone loss. Treatment with estrogen tends to slow down but not reverse osteoporosis. Estrogen replacement therapy works by reducing bone resorption, the process by which bone is broken down to release minerals, such as calcium, from the bone into the blood stream. Use of the hormone, however, is controversial because of the potential for increased risk of uterine cancer, breast cancer, stroke, heart attack and other complications. Taking progesterone in combination with estrogen does reduce the risk of uterine cancer. Because of the documented side effects, the US Food and Drug Administration (FDA) recommends that women consider using estrogen treatment only if they are at high risk of osteoporosis and can’t take non-estrogen medications. It is also important that estrogen-treated women receive regular gynecologic and breast examinations, including mammography before and regularly during estrogen therapy.
Nutrient Supplements
Several researchers have studied the effects of treatment with calcium supplements with and without vitamin D, again with variable results. As with estrogen therapy, results generally show that such treatments slow down but do not reverse osteoporosis once it develops. Further, hypercalcemia (high blood calcium) has been shown in some studies using vitamin D to increase calcium absorption.
Physical Activity
Physical activity is an important part of osteoporosis treatment. Movement that causes the body to work against gravity facilitates the flow of calcium to the bones and the maintenance of bone density. People deprived of physical activity, such as those immobilized in bed, have a dramatic loss of bone mineral. Likewise, physical activity that increases both gravitational and muscular stress in bone has been found effective both as a preventive and rehabilitative therapy for bone loss in people with osteoporosis. This type of physical activity is often referred to as weight bearing exercise. It is important to take care when walking or participating in other physical activity to avoid unsafe situations that may lead to fractures.
Medications
Along with proper nutrition and weight bearing exercise, your physician may prescribe medications to help prevent and/or treat osteoporosis. Currently, bisphosphonates (alendronate, risedronate, and zoledronic acid), calcitonin, estrogens, parathyroid hormone and raloxifene are all approved by the FDA for the prevention and/or treatment of osteoporosis.
Osteoporosis Prevention
Because of the difficulty in finding a therapy to effectively treat or cure osteoporosis without risk or adverse side effects, a growing emphasis has been placed on its prevention. The goal is to prevent undue bone loss. Exercise and certain dietary measures can help.
Physical Activity
Bones, like muscles, need to be stressed. They must be regularly subjected to weight-bearing and/or weight-resistance exercises and activities such as brisk walking, hiking, jogging, dancing, weight lifting, or playing a racquet sport. Thirty minutes including a combination of weight bearing and weight-resistant physical activity most days of the week will help build strong bones, as well as improve heart health, coordination, and balance. Before starting any exercise program, do consult with a knowledgeable physician about your fracture risk. Also, start slowly and build up to the desired level of daily activity.
Diet
Balancing calorie and nutrient requirements becomes more of a challenge with age. Because of slowed metabolism, nutrient-to-calorie needs increase with age. The estimated energy requirements for women over age 50 range from 1,600 to 2,200 kilocalories daily; and the estimated energy requirements for men over age 50 range from 2,000 to 2,800. Within these levels of calorie intake, certain nutrients must be included if the risk of osteoporosis is to be reduced.
Calcium
One of the most important nutrients in reducing risk of osteoporosis is calcium. Surveys of patients with osteoporosis generally indicate a lifelong diet lower in calcium than seen in age-matched populations without bone demineralization. Metabolic balance studies show that such patients are in negative calcium balance.
When dietary calcium is increased, calcium balance eventually becomes positive, indicating retention of calcium. For maximum calcium retention and to build strong bones, children aged 4 through 8 should get 1,000 milligrams of calcium a day. Children ages 9 to 18 require 1,300 milligrams of calcium per day. For people 19 through 50, 1,000 mg of calcium is recommended daily to maintain calcium balance and reduce the risk of osteoporosis. After age 50, recommended intake increases to 1,200 mg daily.
Unfortunately, calcium consumed daily by Americans is about 30% below the recommended daily amount. While the body can generally adapt to some reduction by increasing the efficiency of absorption, often this is not enough. Also, the ability to compensate decreases with age. This makes getting enough calcium even more important in later years.
Good Sources of Calcium
Milk, yogurt, cheese, and other dairy products are major sources of calcium (Table 1). An 8-ounce glass of milk, for instance, contains approximately 300 milligrams of calcium. That’s one-fourth to one-third of the daily requirement —just from one glass of milk. To keep a healthy heart along with preventing osteoporosis, choose fat-free or low-fat milk and dairy products. If drinking milk is not preferred, include dairy products like yogurt, cottage cheese, and string cheese in snacks and meals throughout the day. One cup of regular, low-fat yogurt includes just as much, if not more, calcium than one cup of milk.
Getting enough calcium can be of special concern for people who are lactose intolerant. This condition occurs in people that have low levels of lactase, the enzyme that digests milk sugar in the intestine. Among dairy products, aged cheeses and yogurt with active cultures often are well tolerated. Lactase enzymes can be added to milk products or taken orally before eating a meal that contains milk or dairy products. Specialty products such as low-lactose milk, ice cream and cottage cheese also are available.
Nondairy sources of calcium include dry beans and fish with edible bones such as sardines and canned salmon. Buy fish packed in water to save calories. If you are monitoring salt intake, rinse canned fish well with water to remove excess salt. Other good sources of calcium include broccoli and green leafy vegetables like collards, kale, mustard greens and turnip greens. Tofu or soybean curd may be a good calcium source if made with a calcium coagulant such as calcium sulfate. Foods fortified with calcium, such as some orange juices, soy milk, breads, and cereals, may also help provide your body with the calcium it needs.
| Table 1: Calcium-rich foods. | |
| Calcium, mg | |
| 1 c. Buttermilk | 284 |
| 1 c. Milk, whole, low-fat or fat-free | 300 |
| 1/2 c. Cottage cheese, 2% fat | 78 |
| 1 oz. American, process cheese | 175 |
| 1 oz. Mozzarella, part skim, low moisture | 207 |
| 1 oz. Cheddar cheese | 204 |
| 1 oz. Monterey Jack cheese | 211 |
| 1 oz. Swiss cheese | 272 |
| 1/2 c. Ricotta, part skim | 337 |
| 1/2 c. Ice cream, vanilla, regular | 92 |
| 1/2 c. frozen yogurt, soft serve, vanilla | 103 |
| 1 c. Fruit yogurt, low fat | 384 |
| 1 c. Plain yogurt, low fat | 415 |
| 1/2 c. Chocolate pudding, instant mix w/ lowfat milk | 153 |
| 1 c. Pinto beans, cooked | 82 |
| 3 oz. Salmon, with bones, canned | 180 |
| 3.75 oz. Sardines, with bones, canned | 382 |
| 1/2 c. Tofu, calcium added | 204 |
| 1 c. Shredded Chinese cabbage, boiled | 158 |
| 1 c. Collards, cooked | 226 |
| 1 c. Kale, cooked | 94 |
| 1 c. Mustard greens, cooked | 104 |
| 1 c. Turnip greens, cooked | 197 |
| 1 c. Broccoli, chopped, frozen, cooked | 94 |
Dietary Interactions and Calcium Absorption
It’s important to note that calcium values given for foods do not reflect factors, cookedsuch as fiber and oxalate, which may impair the absorption of calcium. Unfortunately, there is little current information on how much of the calcium in foods high in fiber or oxalates actually is available. We do know that only a small percentage of the calcium in spinach, which is high in oxalates, is available to the body. Calcium availability is less of an issue when overall calcium intake is high.
Other dietary factors that increase calcium loss include high intakes of phosphorus, protein, vitamin A, alcohol and caffeine. Protein is an important nutrient, essential for the growth and repair of body cells. But diets high in protein can cause increased calcium excretion. For adult women, 46 grams of protein per day is sufficient; for men, 56 grams. Cigarette smoking also increases calcium loss and may promote the development of osteoporosis.
Vitamin D is needed for proper absorption of calcium. Regular exposure to sunlight, along with drinking vitamin D-fortified milk, will meet the vitamin D needs of most young people. This may not be sufficient for some older people. Supplementation of vitamin D3 (cholecalciferol) to provide vitamin D intakes of 600 to 800 IU per day has been shown to improve calcium balance in elderly people. It is important to take vitamin D supplements under the supervision of a physician or dietitian. Excessive levels (above 2,000 IU per day) can be toxic. Minerals such as magnesium, phosphorus and vitamin K are also important for bone health and usually can be obtained by eating a well-balanced diet.
Calcium Supplements
If you are not able to consume sufficient levels of calcium through diet, your health care provider or dietitian may recommend calcium supplements. The calcium in most supplements is usually in the form of either calcium carbonate or calcium citrate. They are both absorbed equally well with meals, but calcium carbonate is harder to digest than calcium citrate and may cause constipation or flatulence in some people. Most calcium supplements come in 500-600 mg tablets. The body does not absorb large doses of calcium as effectively as it does small ones. So, taking about 500 mg of calcium at a time may be the best option.
Recommended Websites
National Institutes of Health Osteoporosis and Related Bone Diseases National Resource Center: www.osteo.org
MedlinePlus Health Information: www.nlm.nih.gov/medlineplus
National Osteoporosis Foundation: www.nof.org
References
Bolland, M., Grey, A., Gamble, G., and Reid R. (2010). Effect of Osteoporosis Treatment on Mortality: A Meta-Analysis. Journal of Clin Endocrinol Metab. (95)3:1174-1181.
Food and Nutrition Board. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D and Fluoride. National Academy of Sciences, National Research Council. Washington, D.C., 1997.
Howe, TE,, Shea, B,, Dawson, LJ., Downie, F., Murray, A., Ross, C., Harbour, RT., Caldwell, LM., and Creed, G. (2011). Exercise For Preventing and Treating Osteoporosis in Postmenopausal Women (Review). Cochrane Database of Systematic Reviews. Issue 7 Art. No.: CD000333.DOI: 10.1002/14651858.CD000333.pub2.
Mahan, L., Escott-Stump, S., and Raymond, J. (2012). Krause’s Food and the Nutrition Care Process. St. Louise, Missouri: Elsevier Saunders.
Pennington, J. and Douglass, J. Bowes & Church’s Food Values of Portions Commonly Used. 18th ed., Baltimore, MD: Lippincott Williams & Wilkins, 2005.
U.S. Departments of Health and Human Services and Agriculture. Dietary Guidelines for Americans, 2005. Available at: www.health.gov/dietaryguidelines/dga2005/document/.
Watts, N., Diab, D. (2010). Long term Use of Bisphosphonates in Osteoporosis. Journal of Clin Endocrinol Metab. 95(4):1555–
1565.
*J. Haas, Colorado State University Extension specialist, and research associate; L. Bellows, Extension food and nutrition specialist, and assistant professor. 9/98. Revised 7/14.
Colorado State University, U.S. Department of Agriculture and Colorado counties cooperating. CSU Extension programs are available to all without discrimination. No endorsement of products mentioned is intended nor is criticism implied of products not mentioned.
Go to top of this page.


